 Online Prescription Referral Form
Online Prescription Referral Form Download Prescription Referral Form
Download Prescription Referral Form
Pathophysiology
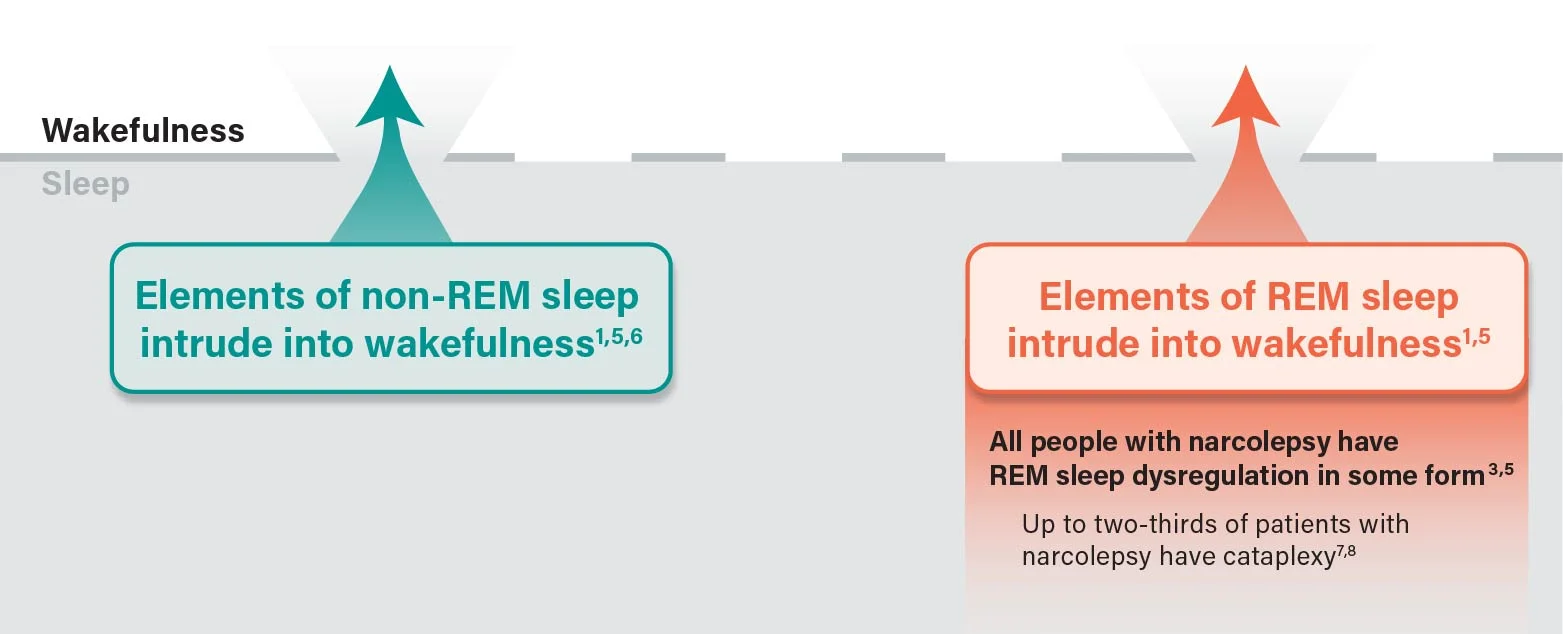
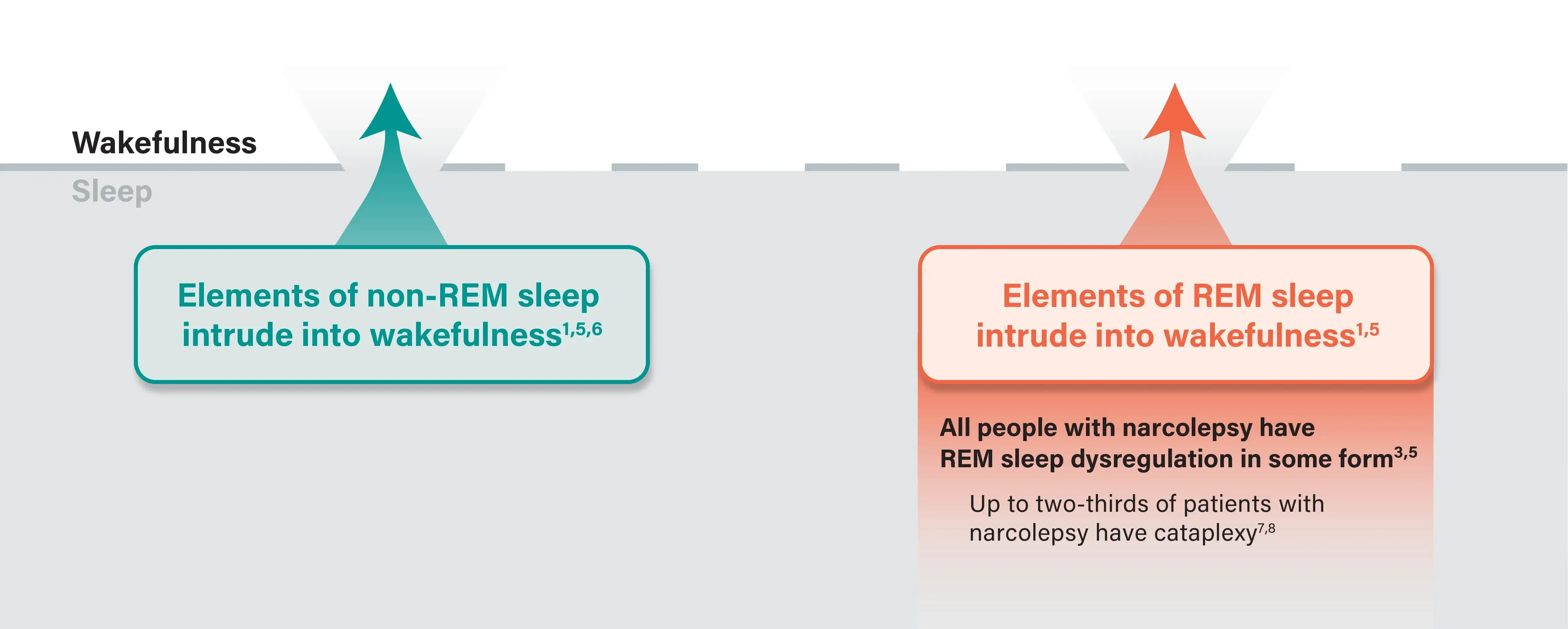
Narcolepsy Is Characterized by Sleep-Wake State Instability1
During the day, unstable wakefulness can occur as excessive daytime sleepiness (EDS) and cataplexy,1,2 the two most common symptoms of narcolepsy3,4
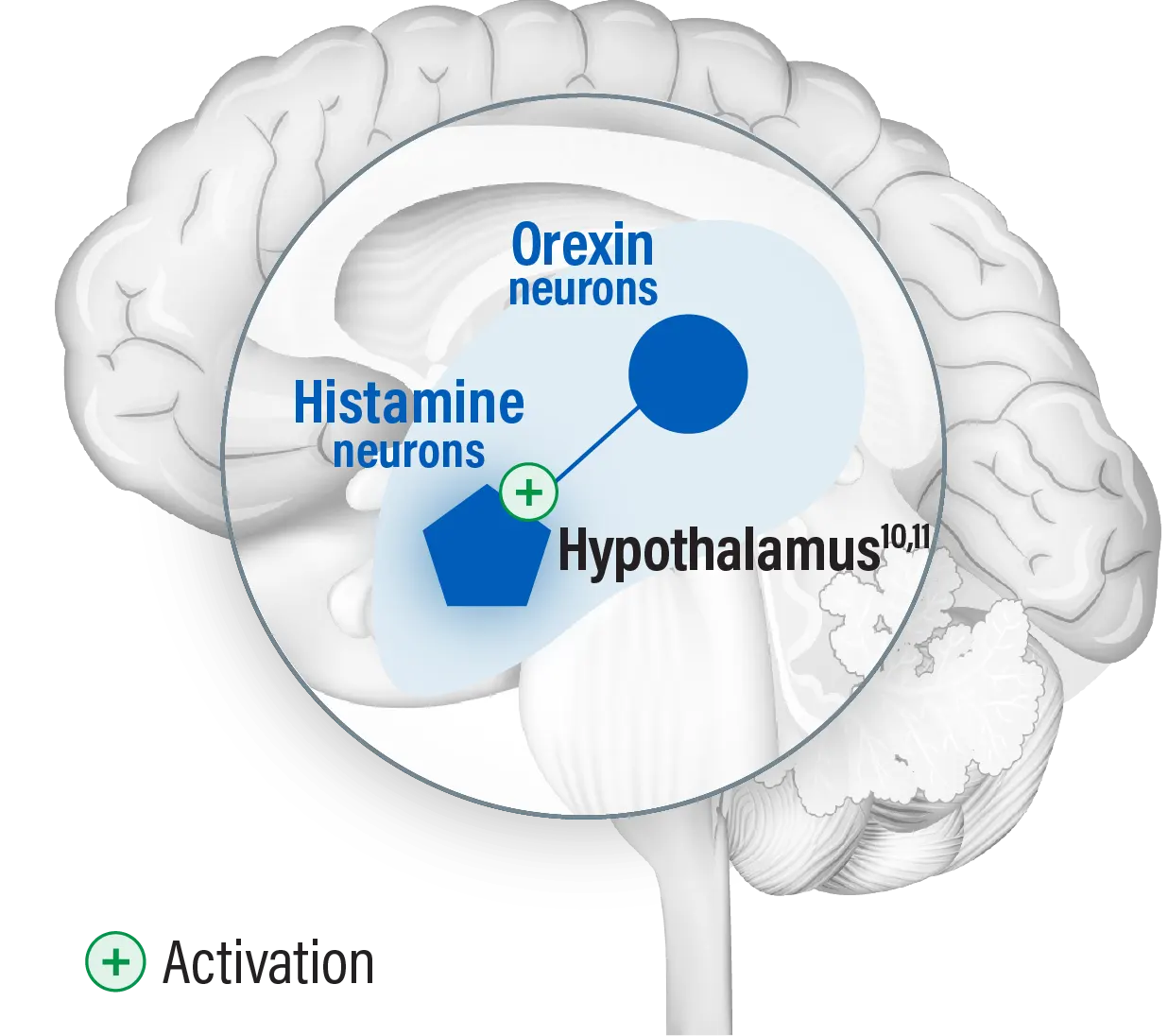
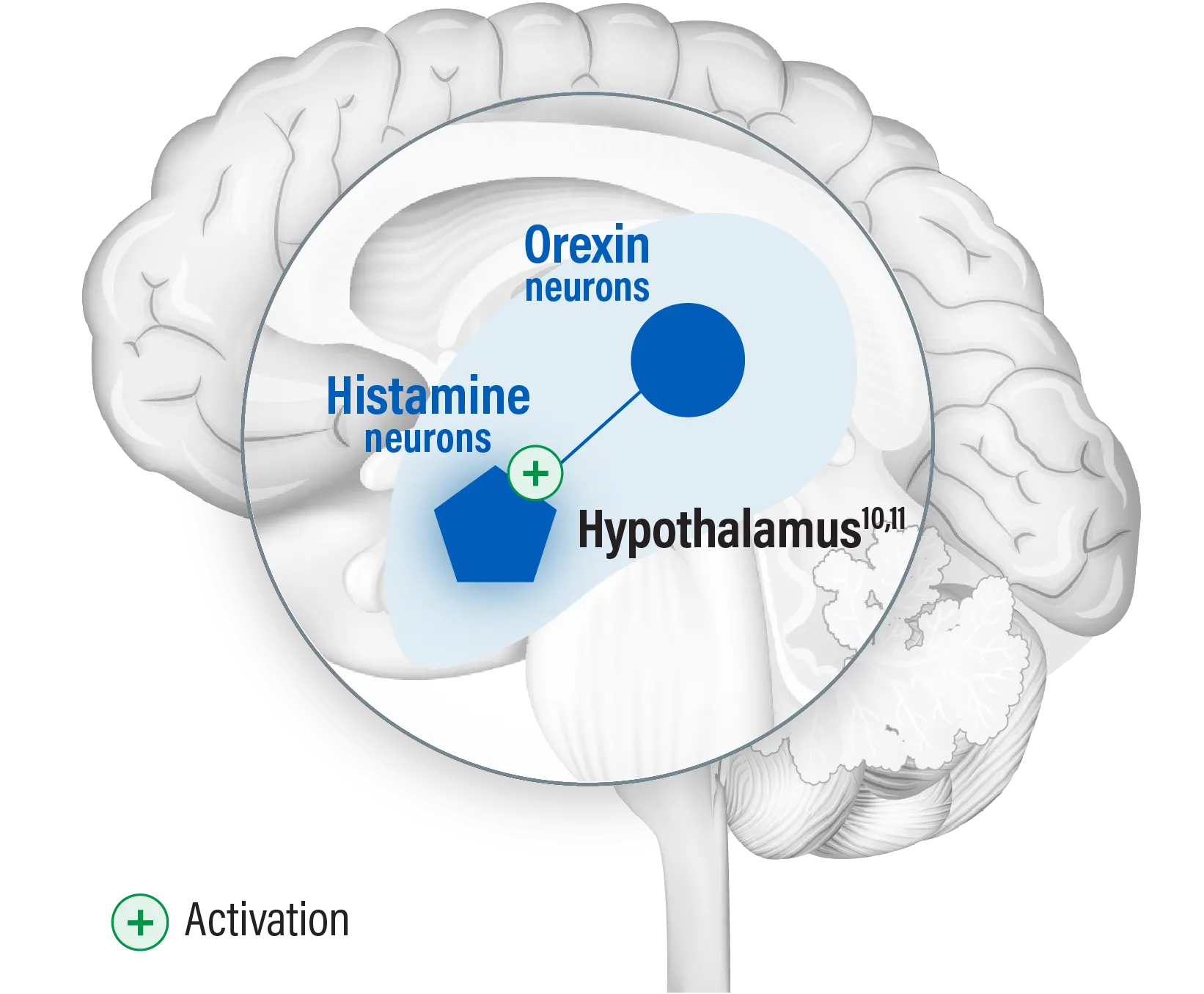
Hypothalamic neurons play a role in regulating the sleep-wake cycle9
Orexin (hypocretin) and histamine neurons both originate in the hypothalamus10,11
- Studies show that orexin and histamine play complementary roles in promoting and stabilizing wakefulness2,10-13